
Peroneal neuropathy, or peroneal nerve damage, refers to any disorder that results from damage to the common peroneal nerve.
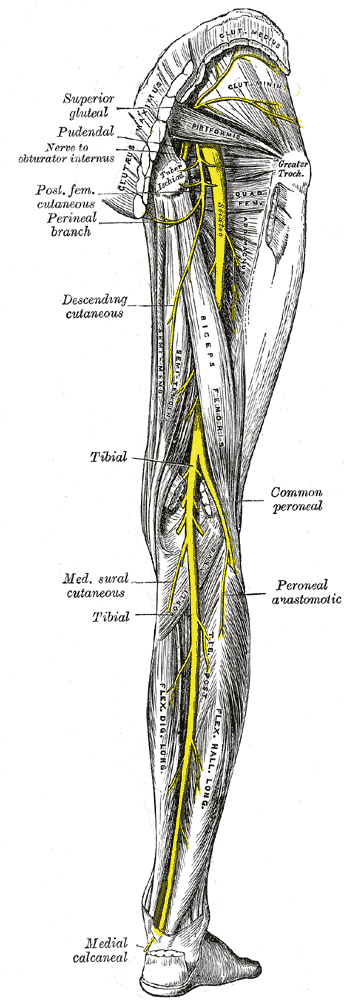
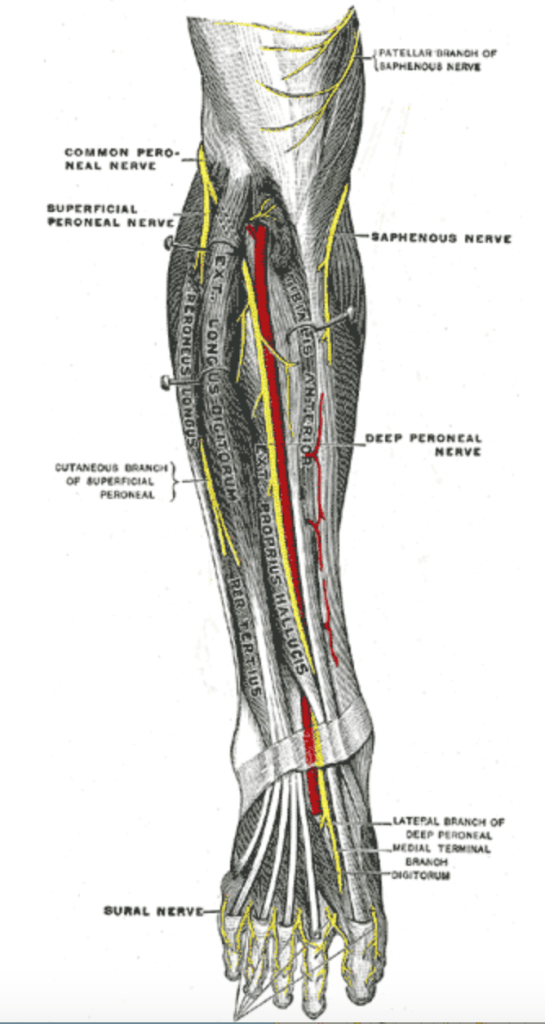
The common peroneal nerve (often just called the peroneal nerve) branches from the sciatic nerve. It provides feeling (i.e. when there is pressure or other sensation) to the front and sides of the legs and to the top of the feet. The peroneal nerve also controls the muscles in the leg that lift the ankle and toes upward, called dorsi flexion.

Mild injuries to the peroneal nerve can cause numbness, tingling, weakness, and pain, all from mild to severe. More severe injuries can cause a gait problem called foot drop, which his a way of walking that results from not being able to bend or flex the foot upward at the ankle. Peroneal nerve damage generally stems from the knee, though can be caused by compression anywhere on the peroneal nerve.
Furthermore, peroneal nerve damage can lead to other injuries. The loss of sensation can lead to accidents, while having weak ankle and foot muscles creates a risk for falling.
Signs of Peroneal Neuropathy
- Decreased sensation, numbness, or tingling in the top of the foot
- Decreased sensation, numbness, or tingling on the outer part of the upper or lower leg
- Weakness of the ankles or feet
- Inability to hold the foot up (foot drop)
- Toes drag while walking
- “Slapping” gait (each step makes a slapping noise when walking)
Diagnosing Peroneal Neuropathy
To diagnose common peroneal nerve damage after childbirth, first and foremost bring up any of the signs written above to your doctor or medical staff, as well as any other issues you are having. Many labor and delivery personnel are not familiar with nerve damage from childbirth so be clear, be firm and advocate for yourself.
Due to this lack of knowledge, many women have not had good support from their OBs and midwives. If this is happening to you, often primary care physicians work well as a primary contact, or if your insurance allows, going directly to a neurologist works well.
After discussing symptoms, your doctor will generally perform a physical exam. Often a neurologist will be called in to do this regardless of what doctor is your principal contact.
To look for weakness, they will test specific muscles that receive sensation from the peroneal nerve. Loss of muscle control in the lower legs and feet. The doctor will look for atrophy of the foot or foreleg muscles; difficulty lifting up the foot and toes; and difficulty making toe-out movements. Another goal of the evaluation is to determine whether the weakness involves only the peroneal nerve or if other nerves are also affected.
Depending on the extent of damage, there are several other or next steps. If you haven’t already been seen by a neurologist, the doctor may recommend it. If you have seen a neurologist, he or she might recommend further testing, described below.
You do not have to see a neurologist. If you need referrals for insurance purposes, your primary care physician can write prescriptions for physical therapy, chiropractic services, acupuncture, massage therapy, devices to assist walking and more. However, the nerve conduction and EMG are performed by a neurologist.
MRI Scan
A MRI scan can look for tumors, growths, or any other masses in the area of the peroneal nerve that could cause compression on the nerve. MRI scans use radio waves and magnets to produce a detailed image of the part of your body that is being scanned. A MRI scan is also used after childbirth to check for damage caused by an epidural, if applicable. This can be requested by a OB, primary care physician, or neurologist.
Nerve Conduction
Nerve conduction checks the speed of electrical impulses in your nerves. An abnormal response, such as a slow time for electrical signals to travel through your nerves, usually indicates damage to the nerve in question. Some find this test uncomfortable or painful, some do not. This is conducted by a neurologist.
Electromyography (EMG)
Electromyography (EMG) is performed after the nerve conduction test. It tests to see how well your muscles and nerves are functioning by recording the electrical activity present in your muscles when the nerves that lead to them are active. The EMG will identify whether the muscle responds correctly to stimulation. Because nerves stimulate and control your muscles, the test can determine problems with both muscles and nerves. This is conducted by a neurologist.
Recovery
- First and foremost, advocate for yourself. Be clear about your symptoms. Do not let any doctor or staff tell you it is normal and to move on.
- Find a doctor who is willing to help you. This could be your OB or midwife. Often it is a primary care physician. Many see a neurologist as well. If one is not helpful or at the least willing to help, move on and find another.
- Get any assisted devices you need. This can be an AFO to help with walking. This can be a wheelchair if you can’t walk at all. This can be a walker or cane. Many progress from a wheelchair, to a walker, to a cane, before walking without any assistance. A shower chair can be helpful as well as a toilet safety rail.
- Set up your space to be with baby in as easy of a way as possible. For example, have everything you need on one floor. Put diaper changing supplies in a basket within easy reach. Put nursing pillow or bottles within easy reach.
- Discuss with your doctor if you should get an MRI to rule out spinal issues.
- Discuss with your doctor if you should get an EMG or Nerve Conduction test.
- Figure out a rehabilitation plan with your supportive doctor. Discuss the following options with her/him:
- Physical therapy – most women with this injury find this most helpful in their recovery. It keeps your muscles from atrophying too much, strengthens them when they do get weaker, and helps nerves reconnect by just trying to use them. If you can’t drive to physical therapy, request in-home services.
- Acupuncture
- Chiropractic services
- Electrical Muscle Stimulation (EMS) – the goal is to strengthen the muscle without involving the nervous system, helping your muscles not atrophy as much when not able to be used; often used at physical therapy.
- Transcutaneous Electrical Nerve Stimulation (Tens Machine) – aims to relieve pain using an electrical current; if having nerve pain, can even use at home.
- Walking
- Water therapy
- Massage therapy
- Stretching
- Foam rolling
- Taking B vitamins
- Be careful – this injury increases your risk of falling. You don’t need further injuries.
- Be patient – nerves take time to regenerate and heal. Then it takes time to strengthen your muscles back to pre-childbirth levels. Just keep putting one foot in front of the other (literally and figuratively!).
- Don’t forget to ask for help! From family, friends or others. This is hard.
Initial Exercises – coming soon
References:
- Peroneal Nerve Injury. John’s Hopkins Medical. 2020 Mar. https://www.hopkinsmedicine.org/health/conditions-and-diseases/peroneal-nerve-injury
- Common Peroneal Nerve. Physiopedia. 2020 Mar. https://physio-pedia.com/Common_Peroneal_Nerve
- Peroneal Nerve. Neurology Needs. 2020 Mar. https://www.neurologyneeds.com/neuroanatomy/peripheral-nerves/common-peroneal-nerve/
- Lipofibromatous hamartoma of the superficial peroneal nerve: Two case reports. Science Direct. “Dermatologica Sinica.” 2012 Mar. https://www.sciencedirect.com/science/article/pii/S1027811711000863#fig3
- Common Peroneal Nerve Dysfunction. Medline Plus. 23 June 2019. https://medlineplus.gov/ency/article/000791.htm
